







OIG CHECK FAQS
What is an OIG check?
An “OIG check” is the process of ascertaining whether a particular individual or entity is found on the HHS Office of Inspector General’s List of Excluded Individual/Entities (LEIE). Excluded individuals are prohibited from receiving reimbursement, either directly or indirectly, from any federally-funded health care program such as Medicare, Medicaid or SCHIP.
This database is updated monthly by the OIG and contains the list of all individuals and entities who are currently prohibited from participating any federally funded health care program. The OIG has the authority to exclude individuals and entities pursuant to section 1128 of the Social Security Act (Act) (and from Medicare and State health care programs under section 1156 of the Act).
The LEIE, also known as the “OIG Exclusion List,” should be checked using the OIG exclusion check process. For more basic information about this list, please see the linked Streamline Verify article.
Who needs to perform OIG checks?
With rare exception, virtually all health care organizations and vendors receive some federal funds related to services and supplies provided to federal health care program enrollees. This includes reimbursement either directly from a federal program or as a subcontractor. The prohibition applies to individuals or entities receiving payment on any basis from federal health care programs, including fee- for-service, contracted or capitated payment. Therefore, hospitals, health plans, provider groups, home health agencies, hospices, rehab facilities, as well as pharmacies, medical transportation companies and durable medical equipment agencies (to name just a few) need to routinely perform OIG exclusion checks to assure that none of their employees, contractors, vendors, interns or even volunteers are on the LEIE.
- What information does an OIG check give you?
What information does an OIG check give you?
Using the OIG’s online Searchable LEIE Database, searching for excluded individuals named “John Smith” produced these results:
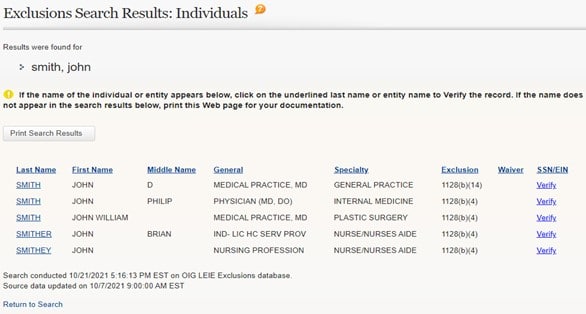
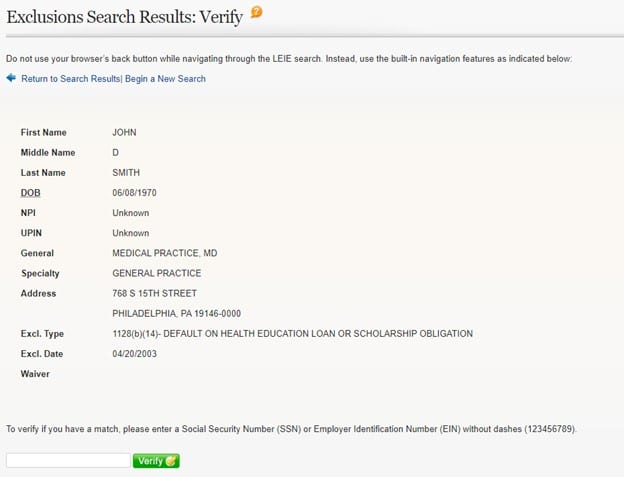
For more information about an excluded individual and the reason for the exclusion, click on “Verify”. Below is an example of the detail provided:
The simple example above does not necessarily reflect some of the challenges of using the LEIE. Because the Online Searchable Database and the Downloadable Database include only the name known to OIG at the time the individual was excluded, any former names used by the individual (e.g., maiden name, previous married name, etc.) should be searched in addition to the individual’s current name. There is no cross-reference function in the LEIE to other databases to check aliases and other previously used names. Also, an individual with a hyphenated name should be checked under each of the last names in the hyphenated name (e.g., Jane Smith-Jones should be checked under Jane Smith and Jane Jones, in addition to Jane Smith-Jones).
Do I need to do both an OIG check and state exclusion list screening?
Yes. The OIG Exclusion List includes state exclusion data which is supposed to be submitted monthly to the OIG. In reality, some states report only sporadically. Even states that report regularly may submit data months after the conviction dates which trigger state exclusion. Under the Affordable Care Act Section 6501, if one state excludes an individual or entity from participation in that state’s Medicaid program, all states are required to exclude the individual. Therefore, the only way for an employer to assure that a potential or current employee is currently not excluded at the federal or state level is to check both resources. Employers are also required to screen regularly against the GSA’s SAM.gov database; to learn more about how the LEIE and SAM.gov differ, please see the linked article.
How do you verify whether the OIG check results match the person you are researching?
As shown on the “Exclusion Search Results: Verify” screen above, list users can verify a match by entering a provider’s SSN or EIN. However, as noted on the OIG’s “Quick Tips” page about how to search the LEIE, the search functions are quite limited. Therefore, if you do not initially find a match, additional research in other federal or state databases may be required.
The time and staff resources for a provider, hospital or health plan to regularly screen against just these the LEIE and state exclusion lists, plus the GSA’s SAM.gov, is considerable and not cost-effective for most organizations. Search findings can be ambiguous, requiring increased staff resources to rule out potential “false positives”. For example, a name on the LEIE may be similar to that of provider but differs enough to rule out a clean match. These require further work and investigation to resolve ambiguities which can be very time consuming. For the reasons states above, monthly monitoring against the LEIE as well as the other required lists can be a daunting and never-ending process that can leave your organization vulnerable to reimbursement and staffing problems.
From a business perspective, contracting with an organization that specializes in exclusion screening, like Streamline Verify, supports both contract compliance and avoidance of potentially significant fines. In addition, having this monthly process performed by an organization that specializes in the review process can save the time of your staff resources and eliminate the worry over potential fines lurking in updated LEIE each month. Streamline Verify clients report that on average, they are able to reduce staff workloads related to monitoring activities by 60%.
Using its propriety exclusion software, Streamline Verify can automate the monthly monitoring functions against the LEIE, SAM.gov and state exclusion databases. Streamline Verify also offers screening capabilities against other sanction lists and licensing lists. Advanced search functionalities match name variations and NPIs against all exclusion databases, so that no potential matches are missed.
How frequently should employers check the OIG’s List of Excluded Individuals and Entities (LEIE)?
The LEIE should be checked prior to extending an offer to any potential hire. Following hire, employers and contracting entities should check the LEIE for all current employees, contractors, vendors, interns and volunteers each month to prevent the continued employment of excluded individuals or entities. The OIG updates the LEIE each month. Failure to check monthly exposes an organization to potential breach of contract claims, civil monetary penalties and other administrative actions by state or federal authorities.
Exclusion applies to more than direct care providers. Therefore, the monthly check of employees, contractors, and vendors against the current LEIE must not be limited to healthcare professionals primarily concerned with patient care. This review process should also include employees providing support services as well as administrative staff and managers. It does not matter if they do not have any interaction with patients. If such excluded individuals are connected to a business which is participating in federal or state healthcare programs, there is a potential violation of the law every time they carry out their functions in relation to that business.
Many state Medicaid contracts expressly require that the LEIE be checked monthly to assure that no excluded individuals or entities serve or receive reimbursement for services provided to Medicaid enrollees. Medicaid contractors may be deemed to have knowledge of exclusion whether or not they check monthly. It should be noted that the ACA extended the reach of Medicaid exclusions through Section 6501 which prohibits any state from allowing an excluded Medicaid provider in one state from participation in Medicaid in any other state. To assure that your organization has not been added to a federal or state list in error, it is prudent to screen your own organization, its business names and its subsidiaries to avoid unwelcome surprises.
Does the OIG List include any history of prior exclusions?
The OIG list is intended to reflect only individuals and entities that are currently excluded from participation in government healthcare contracts. The LEIE also does not reflect reinstatement dates for those individuals and entities who apply for and are granted reinstatement. However, reinstatement is not automatic and is not guaranteed.
Exclusion information is available to LEIE users in several forms. The full LEIE Database updated monthly is a complete inventory of all individuals or entities currently under exclusion and can include information that stretches over many years. The Monthly Supplement files contain only the reinstatements for one month or the exclusions for one month. The Reinstatement Supplement contains information not captured in either the full LEIE database or the monthly exclusion supplement. These monthly reinstatement files contain valuable information for potential employers to identify previously excluded parties when making hiring decisions. While employers can hire individuals or entities previously excluded, they may wish to better understand the prior actions of a potential hire that resulted in exclusion.
The OIG Exclusion List and the CMS Preclusion List - are they related?
Yes, they are, but they are not entirely consistent.
The Preclusion List, updated monthly, provides the name of providers and prescribers who are precluded from receiving payment for Medicare Advantage (MA) plan items or services, or Medicare Part D drugs furnished or prescribed to Medicare beneficiaries. This payment limitation applies to MA plans, Medicare Cost plans and Programs of All-Inclusive Care for the Elderly (PACE) plans and Medicare Part D plans. Effective April 1, 2019, MA plans were required to deny payment for a health care item or service furnished by an individual or entity on the CMS Preclusion List and Part D plans were required to reject a pharmacy claim (or deny a beneficiary request for reimbursement) for a Part D drug prescribed by an individual on the Preclusion List.
The CMS Preclusion List is comprised of any individual or entity that meets the following criteria:
- Is currently revoked from the Medicare program and is under an active reenrollment bar, and CMS has determined that the underlying conduct that led to the revocation is detrimental to the best interests of the Medicare program;
- Has engaged in behavior for which CMS could have revoked the individual or entity to the extent applicable if they had been enrolled in Medicare, and CMS determines that the underlying conduct that would have led to the revocation is detrimental to the best interests of the Medicare Program, or
- Have been convicted of a felony under federal or state law within the previous 10 years that CMS deems detrimental to the best interests of the Medicare program.
The Preclusion List can include not only individual medical practitioners and providers, but also dentists, pharmacists, pharmacies, medical practices and medical suppliers. In addition, providers who voluntarily opt out of Medicare will appear on the Preclusion List.
How These Lists are Related
Use of the CMS Medicare Preclusion List does not eliminate the requirement that Medicare Advantage and Part D plans validate their providers monthly against the OIG’s LEIE. This list is updated monthly by the OIG to reflect exclusions from participation and payment under Medicare or Medicaid contracts due to criminal behavior.
There is indeed substantial overlap between the lists but they are not entirely consistent:
- Providers excluded by the OIG’s LEIE will be on the CMS Preclusion List. OIG exclusions are imposed due to criminal behavior and as such are part of the CMS Preclusion List criteria. Therefore, if a plan finds a provider in the OIG LEIE, the plan is not required to check the CMS Preclusion List.
- However, there are other providers who are precluded by CMS from participation in a Medicare plan and yet will not appear on the OIG Exclusion List because the preclusion is based on other criteria. In that case, a MA or Part D plan should check the CMS Preclusion List as well.
An additional factor to consider is why a provider was excluded or precluded. Once a provider is removed from the OIG’s LEIE and is no longer excluded due to a reinstatement by the OIG, a MA and Part D plan must then turn to the CMS Preclusion List because there are instances in which a provider remains precluded by CMS from plan participation even though they are no longer excluded by the OIG. For example, CMS may bar reinstatement from Medicare plan participation or perhaps the provider was precluded for behavior which CMS deems sufficiently problematic to warrant being removed from participation in a Medicare plan even though it did not result in a criminal conviction.
Another difference between the two lists is data capture. Unlike the OIG’s LEIE list which deletes the names of providers who are reinstated or have completed their period of exclusion, impacted providers will not drop off the CMS Preclusion List. Instead, the updated CMS List will indicate a reinstatement date that an impacted provider is no longer precluded.
The OIG issued a notice in 2022 that it considered whether to discontinue its publication of monthly supplements to the LEIE but as of December 2022, these are still available.
How do individuals or companies end up on the OIG exclusion list?
There are many reasons that an individual or organization can be excluded, as explained in some detail on the HHS OIG website as well as industry issuances.
Most exclusions by the OIG start with a state’s report of a felony or misdemeanor criminal conviction or due to professional misconduct that resulted in sanction of a provider/entity by a state licensing board. For example, a nurse whose professional license is revoked (or voluntarily surrendered) due to a quality of care issue or drug abuse charge will be subject to exclusion at the federal level. States are required to notify the OIG of such actions taken.
There are two types of exclusions that the OIG can impose. The misconduct or criminal action dictates which type of exclusion applies:
- Mandatory Exclusion. If an individual/entity is convicted of the following criminal offenses, the OIG is required by law to impose a minimum 5-year term of exclusion. The OIG has no discretion on decisions to exclude in cases that meet the statutory exclusion standards that include
> Health care fraud related to Medicare, Medicaid, SCHIP, or any state’s healthcare program;
> Patient abuse or neglect; and
> Felony conviction under Federal or State law relating to fraud, theft, embezzlement, breach of fiduciary responsibility, or other financial misconduct in connection with the delivery of a health care item or service. - Permissive Exclusion. Unlike mandatory exclusions, the OIG has some discretion when imposing permissive exclusions and the term of exclusion. Permissive exclusion generally involves misdemeanor criminal convictions, as well as other lesser offenses, including default on student loans.
If an OIG check results in a match, what should we do?
For smaller organizations who have a limited number or employees, providers and contractors, conducting the OIG exclusion check, which involves checking the OIG Exclusion List, may seem like a quick monthly exercise. Simple exclusion screening searches are done as follows: The employer inputs the employee’s (or potential hire’s) name, date of birth into the database. The database returns a list of potential matches, including individuals with similar names. The employer must then independently verify whether or not the employee in question is, indeed, the same person as the excluded individual. Employers are also required to check all versions of each employee’s name, including maiden names, combined names (i.e., Smith-Jones; Smith; and Jones), and name diminutives (i.e., Robert/Bob).
If you have all of the identifiers needed to definitively rule out any false positive or false negative potential matches, and have a very stable employee and contractor base, then how could there be a change in status from one month to another? In short, changes can be noted from month to month due to a number of factors, including delays by the OIG to upload information from the state Medicaid programs (which routinely submit updated exclusion information months late), delays by states to update their Medicaid exclusion lists, provider name changes or clarifications, and reinstatements into the Medicare program going into effect.
If an organization chooses to pursue in-house exclusion checking, it needs to establish a dedicated resource who will not only check the LEIE and the GSA’s SAM List as required by contract, but also be prepared to research other databases such as state Medicaid exclusion lists (Medicaid providers), the CMS Preclusion List (for Medicare providers), state licensing board actions, as well as cross-checking provider identifiers such as their EIN or other national databases when names or information noted in the LEIE do not appear to clearly eliminate a potential match. Checking state exclusion databases is necessary because individual states may exclude individuals for reasons other than the ones cited by federal law, without immediately reporting to the OIG or to other states. The only way for employers to ensure compliance with the mandated requirement is to conduct a nationwide search each and every month.
The complexity of the monthly OIG checking process for all organizations is daunting and very time intensive. To avoid failing to identify an excluded individual or entities, healthcare contractors often leverage the expertise of organizations such as Streamline Verify which have created proprietary software to compare information across all relevant databases and exclusion lists. By engaging a contractor to perform the required checks on a monthly basis, healthcare organizations can use their internal resources to address any potential matches that Streamline Verify has extensively vetted across multiple lists. This is a much more cost-effective approach that also guarantees a consistent monthly check to assure that an organization is not risking potential exposure to fines, penalties and findings.





















