







Streamline Verify has worked many organizations in the healthcare industry during our many years in business. In addition to health plans, hospitals, universities and physician groups, we are privileged to include among our clients many other specialty groups and organizations.
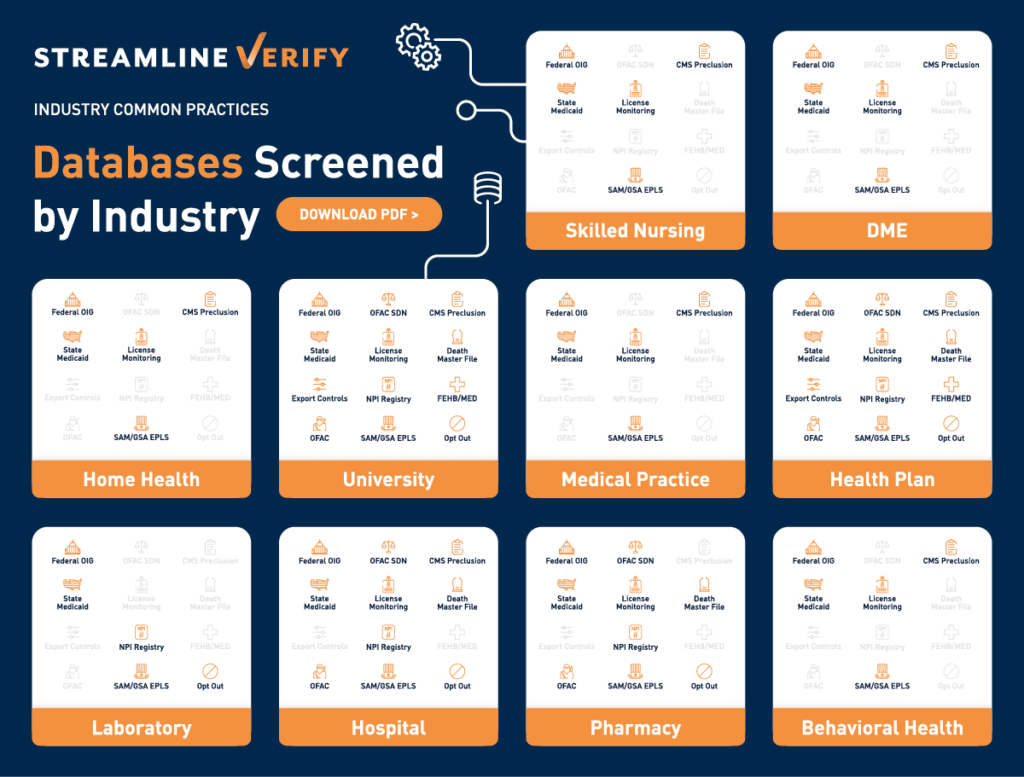
While there are many commonalities in terms of exclusion and sanction screening across various organizations, we have noted differences in industry practice as well. Streamline Verify recently developed a infographic capturing which databases are screened as a matter of common industry practice across various types of health care organizations. Of course, this overview would not apply to those rare organizations that do not (either directly or indirectly) receive federal funding for services rendered. Also, it should be noted that there may be organizations that receive federal funding as a Medicare contractor or downstream entity, but do not participate in Medicaid or the federal employee health plan (FEHP). Therefore, the types of screening by sector may differ from organization to organization based on participation in federal programs.
Commonalities Across Sectors
As you will note upon review, all industry sectors screen regularly against the federal OIG list also known as the List of Excluded Individuals/Entities (LEIE), the GSA’s SAM.gov database, and the state Medicaid exclusion lists. Sectors also monitor the professional licensure status of their staff.
To recap each of these lists:
- The LEIE is the exclusion list maintained and published monthly by the HHS-OIG of all currently excluded individuals and entities, who are ineligible to receive any federal funding for health care services rendered to government program beneficiaries. Exclusions are applied in the event of criminal convictions and significant professional misconduct. The duration of the exclusion differs based on the nature and severity of the criminal behavior and misconduct. Exclusion by the OIG is the most severe civil penalty that can be imposed for such misconduct. The LEIE is the primary source of exclusion data for the health care industry.
- The SAM.gov is a database maintained and published by the General Services Administration (GSA) and reflects the sanctions, exclusions and debarments taken by multiple federal agencies. It is the primary database to check against for all federal contracting and procurement. Unlike the LEIE which is focused on health care exclusionary actions, SAM.gov reflects actions that impact multiple industries.
- Most states maintain a state-specific Medicaid exclusion list. States are required to report all Medicaid exclusions to the OIG for review for inclusion in the LEIE. States that do not maintain a separate searchable list instead rely on the LEIE. As a result of the Affordable Care Act section 6501, exclusion by one state Medicaid program requires exclusion from all other state Medicaid programs. For this reason, state Medicaid exclusions are a critical screening for organizations that receive federal funding, either directly or indirectly.
- Professional licensure that is current and in good standing dictates whether a medical professional can perform and bill for their services. Therefore, organizations both initially credential and then periodically re-credential their licensed professional staff to validate the status and currency of professional licensure.
Where Differences Emerge
Aside from these four commonalities described above, the infographic shows the significant divergence in screening across industry sectors. Not surprisingly, health plans, hospitals and universities screen most extensively due to:
- regulatory mandates
- their contractual arrangements with state and federal agencies such as CMS and Medicaid programs
- the types of licensed professionals with whom they subcontract for services.
The specialty sectors differ widely in terms of screening practices. For example, while pharmacies screen extensively against multiple databases, the screening performed by other specialty healthcare organizations such as DME vendors, laboratories and home health companies is more limited. Pharmacies are subject to a myriad of state and federal regulations controlling the distribution of medications, particularly as relates to controlled substances.
OFAC
The U.S. Office of Foreign Asset Control (OFAC) is the department of the U.S. Treasury that is responsible for facilitating compliance with the U.S. foreign policy and national security agendas. OFAC works to bring those involved in narcotics, terrorism, and other undesirable activities that threaten U.S. national security into line. OFAC administers a number of different sanction programs to address both individuals and companies owned or controlled by, or acting on behalf of, targeted countries as well as individuals, groups and entities (including terrorists and drug traffickers) designated under programs that are not typically specific to a particular country. The OFAC Specially Designated Nationals and Blocked Persons List (“OFAC SDN List”) has approximately 6,300 names connected with sanctions targets.
U.S. individuals and organizations are prohibited from dealing with SDNs. Sanction targets found on the OFAC SDN list change frequently and therefore, it is very important to check OFAC’s website regularly. As an employer, checking the list prior to hire is not specifically required, but hiring someone on the list is prohibited. It should be noted that when an employer does find a potential match on the list, it is required to notify OFAC. Compared to the other federal exclusion lists such as LEIE and SAM.gov, the possibility of a potential contractor or employee appearing on the OFAC sanctions list is less probable. Nonetheless, failing to check and then contracting with anyone on an OFAC list can lead to consequences that outweigh taking the extra time to screen against the OFAC list.
CMS Preclusion vs Medicare Opt-Out
It should be noted that the CMS Preclusion List is only accessible by Medicare Part C & D health plans, Medicare Cost plans and PACE programs. The CMS Preclusion List must be checked by health plans which offer these Medicare programs. While there is overlap between the CMS Preclusion List and the LEIE, these lists are not wholly concentric because the criteria for inclusion on each differ. Therefore, both lists must be checked by health plans participating in these Medicare programs.
On the other hand, the Medicare Opt-Out List is publicly available. This list, maintained by CMS, also is critical to medical practices that treat Medicare patients, since services by provider who has either voluntarily opted out of Medicare participation cannot bill a Medicare managed care program.
Death Master File
Another database that is commonly screened by larger organizations such as health plans, hospitals, and universities as well as pharmacies is the Social Security Administration’s Death Master File (DMF). This file is the primary federal repository of all deceased persons in the U.S. The DMF (also known as the Social Security Death Index or “SSDI”) is a searchable database updated monthly and weekly which contains over 94 million records of deaths of individuals who had SSNs and in its current form is searchable back to 1962.
The Social Security Administration relies on multiple data sources to populate the Death Master File, including financial institutions, federal/state agencies, postal authorities, decedents’ families, health care organizations, and funeral homes. There can be a lag in reporting that affects the currency of the information available. Social Security does not guarantee 100% accuracy of the DMF data so a DMF search cannot be used to definitively validate that a person is alive.
The Death Master File is a bulwark against fraud for organizations that are billed for medical services. Unfortunately, there are billing schemes where fraudsters submit claims on behalf of deceased providers and individuals for bogus services. Screening claims against the Death Master File can prevent plans and state/federal programs from inadvertently paying out on behalf of deceased providers and patients.
NPI Registry
National Provider Identifiers (NPIs) were created to ensure for accuracy and efficiency in the health care system when it comes to transmitting information that references healthcare providers and organizations electronically, with an aim to help reduce fraud and abuse. NPIs do not encode any information about the given health care provider; they are purely an identifier. CMS maintains a searchable registry database of all NPIs issued.
Commercial insurers use these 10-digit NPI numbers to conduct NPI provider searches. In addition to use in electronic transactions, electronic medical record systems may use NPIs in patient records, where a treatment facility or physician of record is identified, or any time legal identification is required, for that matter. And most importantly the OIG updates updating their exclusion lists with NPI numbers, making the screening process far more accurate.
Export Controls
This category of databases includes export-related restricted, denied, and blocked persons lists issued by the US Departments of State and Commerce such as Department of State Non-Proliferation Orders related to missile sanctions, chemical & biological weapons sanctions, as well as the transfer of Missile Sanctions. While these are similar to the OFAC list in that these lists are less likely to yield a match, there are healthcare organizations such as universities and health plans that do routinely screen against these.
Conclusion
Streamline Verify works with each client to customize screening of their employees and contractors against state and federal databases as required to confirm that their workforce members are not excluded, suspended or otherwise ineligible to participate (directly or indirectly) in any federal healthcare program. As this infographic clearly shows, the number and complexity of screening obligations is daunting. However, as an expert in the screening field with a proven track record of success across multiple sectors of the healthcare industry, Streamline Verify can perform all required screenings on behalf of its clients to produce actionable reports related to any potential findings. Allowing an expert to take on this process can relieve internal staff resources of the frequent monitoring required of organizations that participate in federal healthcare programs and will produce consistent results that are verifiable from month to month.

























